Please choose from the menu options or select the option to type
in your own text. Thank you!
Medical History
Please choose from the menu options
Eye History
Medical history
Review Of Systems
*Check all that apply
Family History
Social History
*This field is required
COVID-19
If you are having any symptoms of being sick, please reschedule your appointment or
speak to a staff member.
Office Policies/Financial Agreement
OUR MISSION: To strengthen our community by enhancing our citizen's sight and improving
their total
health by delivering personal care.
OUR PROMISE: As your trusted eye care professionals, our promise is to always recommend
and offer to you our coveted patients the best medical treatments and options available
despite the uncertainty of the insurance marketplace and coverages they may offer.
WELCOME: If you are a new patient to us or even returning patients who desire to be fit
with eyeglasses or contact lenses, please be prepared for your visit to take 1 to 2
hours on average depending on your needs. We do our utmost to respect each individual's
time, however we practice personalized health care and unexpected problems occur that
occasionally will interrupt our schedule which could possibly cause you delays. Please
accept our sincere apologies if you get delayed. Please help us by allotting appropriate
time in your schedule and communicating to us anytime constraints you may have, so we
may effectively serve your individual needs. If delays occur please discuss with us any
time limitations you have, so we can expedite your visit or reschedule your appointment
if necessary.
CANCELLATION/MISSED APPOINTMENT POLICY: Please kindly give us 48 hour notice if you cannot
make your appointment. We have set aside time to meet your needs at your appointed time and
therefore we have made that time unavailable to others. It is important to us to help as
many patients as possible in meeting our mission to strengthen our community. We consider 15
minutes after your appointed time to be a missed appointment. If you truly have an emergency
arise that will prevent you from making your appointment, please alert us as soon as
possible. We have adopted the following policy for all other missed appointments: First
missed appointment will result in a reminder and review of this policy. Second and all
future missed appointments will result in a $50 fee to cover administrative costs. This fee
cannot be covered by insurance. Thank you for your cooperation.
SERVICES: Medical eye care services vary widely based on the services performed. These
services may incur additional costs to your vision exam or may change a vision exam to a
medical exam as we determine what services are necessary for your situation. The total cost
of your exam may not be known until the conclusion of the exam. Examples of medical services
include but are not limited to management of cataract, glaucoma, floaters/flashes, ocular
allergies, dry-eye syndrome, diabetic ocular complications and foreign body removal.
Vision exams are for those seeking eyeglasses or contacts. A contact lens fitting is
additional
and can vary depending on the type of lenses and amount of service required for a
successful fit. An
exam is often required to determine the type of fit necessary. It is noteworthy, most
vision plans
will not cover both glasses and contact lenses or fitting fees.
Refraction is the portion of the eye exam that allows the Doctor to determine your need
for vision
correction and is necessary for a glasses or contact lens prescription. Vision insurance
benefits
routinely cover this service as part of a vision exam, however Medical insurance does
not and will
typically incur an additional fee to you.
|
Do you want to be checked for a new eye glasses prescription?(May create a
$65 charge with using medical insurance only.)
|
*This field is required
|
Initials:
*This field is required
FINANCIAL: To best serve you, it is necessary for you to provide any and all benefits prior
to your examination. This includes Medical and/or Vision Insurance benefits and any
discounts or certificates you wish to apply. In order for us to apply ANY medical or vision
insurance benefits we will need your full social security number at the time of scheduling
the appointment. If you feel uncomfortable giving this information over the phone, we
understand but will need it at the time you arrive for your appointment. Further, we ask
that you advise us prior to
examination of your desire to use a given plan or benefit. We do our best to inform you of
your benefits and assist you in applying them.
However, IT IS YOUR RESPONSIBILITY TO KNOW YOUR INSURANCE BENEFITS AND REQUIREMENTS
INCLUDING IF YOUR BENEFITS REQUIRE A PRIOR REFERRAL OR PRE-AUTHORIZATION. YOU MUST
PROVIDE/FACILITATE REFERRALS FROM YOUR PRIMARY DOCTOR OR CONFIRM WE HAVE SECURED REFERRALS
AND/OR PRE-AUTHORIZATIONS 2 BUSINESS DAYS PRIOR TO YOUR APPOINTMENT OR THE COST OF SUCH
SERVICES MAY BECOME YOUR RESPONSIBILITY.
If you have questions or need to know more about your benefits please discuss your concerns
with us prior to being seen by the Doctor. I understand and agree.
However, IT IS YOUR RESPONSIBILITY TO KNOW YOUR INSURANCE BENEFITS AND REQUIREMENTS
INCLUDING IF
YOUR BENEFITS REQUIRE A PRIOR REFERRAL OR PRE-AUTHORIZATION. YOU MUST
PROVIDE/FACILITATE
REFERRALS FROM YOUR PRIMARY DOCTOR OR CONFIRM WE HAVE SECURED REFERRALS AND/OR
PRE-AUTHORIZATIONS 2 BUSINESS DAYS PRIOR TO YOUR APPOINTMENT OR THECOST OF SUCH
SERVICES MAY
BECOME YOUR RESPONSIBILITY.
If you have questions or need to know more about your benefits please discuss your
concerns with us
prior to being seen by the Doctor. I understand and agree.
Initials:
*This field is required
I have read the above policy regarding payment for services rendered or products provided.
Further, I understand that if insurance is being filed on my behalf, I will need to give my full social security number to the staff and I will be responsible
for co-pays, co-insurance, deductibles, and any other fees my insurance may not cover.
Payment is expected at the time of service unless prior arrangements are made. If you have
questions, please discuss with staff prior to your evaluation.
Initials:
*This field is required
I agree to pay any and all fees accrued from collection companies if my overdue balance
should be sent to such company. Unpaid bills will be sent to a collection company after
90days from the date of service unless prior arrangements are made. I understand that
collection fees may be as much as 33% of my total overdue bill.
Initials:
*This field is required
I hereby authorize payment directly to the Doctor for benefits otherwise payable to me for
services as coded for the exam and/or materials. I understand that I am responsible for the
balance of fees not covered by insurance. Note: any refunds I am due will be made via check
and may require several weeks to process and receive.
Initials:
*This field is required
ACKNOWLEDGMENT OF NOTICE OF PRIVACY PRACTICES
*One selection
below is required
The law requires that Jesse S Hicks, OD, PA/SeePort Optometry make every effort to
inform you of
your rights related to your personal health information. By my signing below, I
acknowledge that
I have read or had explained to me prior
to any
services
offered Jesse S Hicks, OD, PA's Notice of Privacy Practice and agree to continue my care
with Jesse
S Hicks, OD, PA under said terms.
I was given to opportunity to read Jesse
S Hicks,
OD, PA's
Notice of Privacy Practices and declined but wish to continue my care with Jesse S
Hicks, OD, PA
under the terms of Jesse S Hicks, OD, PA's privacy policies.
I have read or had explained to me prior
to any
services
offered Jesse S Hicks, OD, PA's Notice of Privacy Practice and do not wish to continue
my care with
Jesse S Hicks, OD, PA under said terms.
The Notice of Privacy Practice could not
be read
due to the
emergent nature of the care or other reason described as.
* Please choose 1 option
I am the patient being examined today
I am a parent/guardian/power of attorney of the
patient.
I HAVE READ AND UNDERSTAND THIS FORM. I AM SIGNING IT VOLUNTARILY.
Signature
*This field is required
Date
*This field is required
If you are signing as a personal representative of the patient, please indicate your
relationship
AUTHORIZATION FOR RELEASE OF IDENTIFYING HEALTH INFORMATION
I authorize Jesse S Hicks, OD, PA/SeePort Optometry to release health information
identifying me
(including, if applicable, information about substance abuse, mental health conditions,
genetic
information, and HIV infection or AIDS) under the following conditions
Specific information to be released:
Name and address of the Recipient(s):
Recipient 1:
Recipient 2:
Termination date for authorization:
None
Termination date:
*This field is required
It is completely your decision whether or not to sign this authorization form. We will
not refuse to
treat you if you choose not to sign this authorization. If you sign this authorization,
you may
revoke it at any time by contacting in writing, FAX or email the Privacy Official noted
in the
Notice of Privacy Practices. When your health information is disclosed under this
authorization, the
recipient has no duty to protect its confidentiality. The recipient may re-disclose the
information
as he/she wishes.
I HAVE READ AND UNDERSTAND THIS FORM. I AM SIGNING IT VOLUNTARILY.
Signature
*This field is required
Date
*This field is required
If you are signing as a personal representative of the patient, please indicate your
relationship
SPECTRALIS OCT Informed Consent
SeePort Optometry is proud to provide our patients with the most highly advanced
technology
available in retinal screening! Our ability to view your internal retinal health is now
dramatically
improved with Spectralis OCT (Optical Coherence Tomography). Dr. Hicks is concerned
about problems
such as macular degeneration, glaucoma, macular holes/edema, macular pucker or
epiretinal membranes,
and diabetic retinopathy; all of which could lead to partial loss of vision or
blindness.
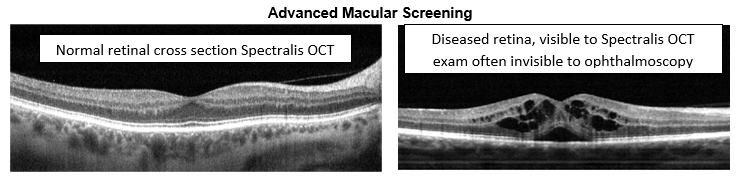
EARLY DETECTION IS CRUCIAL
Spectralis OCT Provides:
• A set of annual eye wellness retinal scans for the macula and for glaucoma
• An in-depth view of the retinal layers (where disease usually starts)
• The ability to show you your images today during your exam
• A permanent record for your medical file, which gives your doctor comparisons for
tracking
and diagnosing potential eye disease
The $39 charge, which would be due at the time of your exam, is typically not covered by
your
medical or vision insurance unless being used to actively follow disease. Dr. Hicks
would like for
ALL patients to have a Spectralis OCT screening annually.
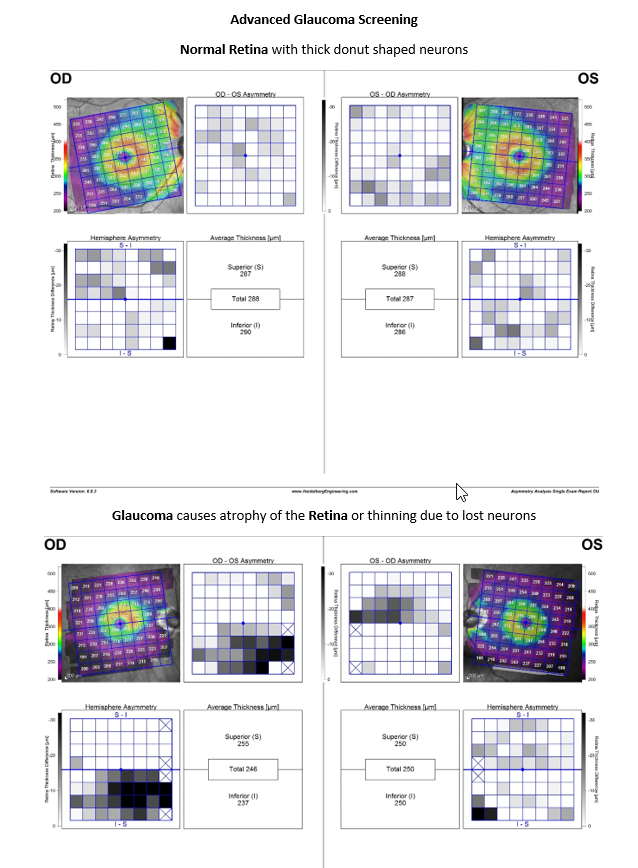
Advanced Glaucoma Screening
Normal Retina with thick donut shaped neurons
Glaucoma causes atrophy of the Retina or thinning due to lost neurons
Please check one of the following: